Dear Readers – please copy this and share it with your own
representatives.
Dear Senators Blumenthal and Murphy and Representative
Courtney,
I am writing this letter with the express intent to goad you
into doing more to prevent the emerging crisis of antibiotic
resistance becoming an urgent public health catastrophe. The most important problem preventing further
progress towards ramping up our antibiotic pipeline is the broken marketplace
for antibiotics. We have come to view these drugs as cheap and always available
– almost like a right to cheap lifesaving medicine. We also like to take new
antibiotics and reserve them for only those patients who absolutely need them
in order to protect them from emerging resistance. This is a good plan for the public health,
but not so much for the marketplace. The antibiotic market no longer provides for even a reasonable return on investment in R&D for these lifesaving medicines.
You may argue that the pharmaceutical companies
make billions in profits every year and that they have an obligation to pay us
back by continuing antibiotic R&D even though they won’t be able to make
money in this area. But these companies are there to make a profit for their
shareholders. They will follow the money.
There are exceptions. But in 1990, ALL of the large pharmaceutical companies
had active antibiotic R&D programs. For those special companies who continue their efforts in antibiotic R&D, given the bleak market prospects, they could abandon their efforts at any time. Some have even been discussing this possibility. Most companies abandoned the area years ago for a
variety of reasons – but the lack of a viable marketplace was an important
motivation.
Why can’t the NIH or academic centers take this on? Because they do not have the resources – but more
importantly, they do not have the expertise. It would take many years of
investment and education to get our academic research centers ready to take on
this task. And even then there are many roadblocks to success here.
Since you have all been involved in discussions around the
regulatory changes needed to assure our pipeline of new antibiotics, I don’t need to explain the importance of the problem
of antibiotic resistance and its potential threat to our aging population as
well as our children and grandchildren. The GAIN Act that forced the FDA to put
feasible antibiotic development pathways in place was an important step. The 21st
Century Cures Act that established a pathway for antibiotics to be used in
limited populations with high medical need was an even more important step and
I applaud you for leading this effort.
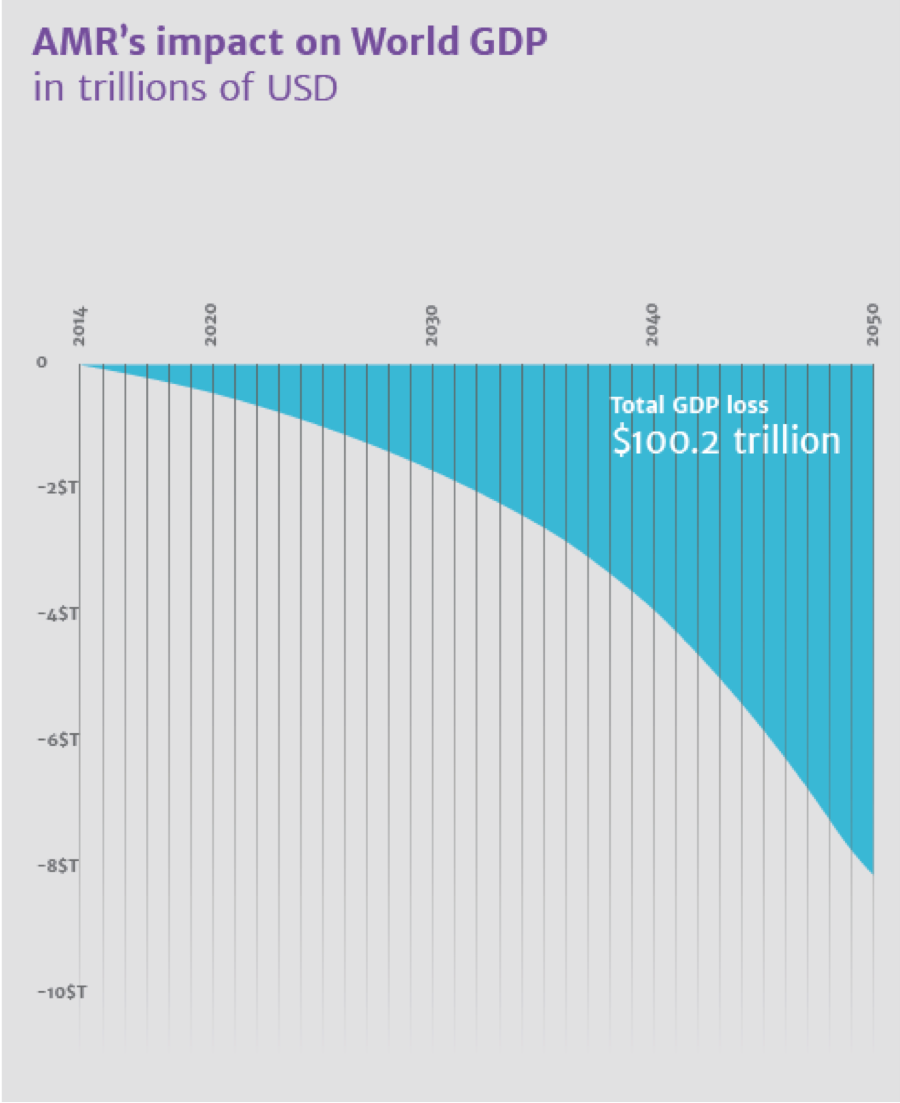
I don’t need to point out that the O’Neill Commission (as I
call it) predicted 10 million deaths worldwide from antimicrobial resistance
(including TB and Malaria) by 2050 if current trends continue. The cost to
society globally could be as high as $100 trillion in lost GDP.

In this crisis the US, including the state of Connecticut is
not spared. Nationally, the rate of highly resistant infections like those
caused by highly resistant Gram-negatives called CRE has been rising as shown
in the following data collected by Achaogen.

The New England area is not spared as shown in this map.

While antimicrobial stewardship and reduction of the use of
antibiotics in agriculture and animal husbandry will help, even appropriate use
of antibiotics will continue to select for resistance. It’s the inevitable result of the formula –
“you use it, you lose it” for antibiotics.
Improved regulatory pathways such as those already in place
and those being developed by FDA will not be the entire answer either.
Why? Because the marketplace for
antibiotics is broken. Only government
can fix this problem. Without a healthy
market, companies, where antibiotic discovery and development expertise reside,
will not invest. They can’t make money
here – especially when compared to areas like oncology. We have seen the result
of this with the majority of large pharmaceutical companies having abandoned
the area starting in 1999.
The push incentives from HHS, the Wellcome Trust and others
have been very powerful in helping to fund antibiotic research and
development. But they still will not be
enough. Companies need to see a viable
market at the end of their R&D road.
The fix, unfortunately, no matter how it is
constructed, will involve spending taxpayer money. The funds can come from all taxpayers, from
consumers of all pharmaceuticals, or from consumers of certain drugs where
generic entry might be delayed by a few months. The way this will work will
depend on the approach that government chooses.
Of course, the other way to fix the broken antibiotic market
is to wait for the crisis to hit. A good example of this is the global pandemic
of methicillin-resistant staphylococcal (MRSA) infection that hit starting
around 1982.

By the late 80s, pharmaceutical companies were increasing their research efforts to come up with new therapies for serious MRSA infections. They did this because they thought they saw a market opportunity in the growing number of cases of these infections. But it took a great deal of time for them to get something on the market. The only oral drug for the treatment of these infections, Zyvox, was approved in 1999. Cubicin, discovered in the late 80s or early 90s hit the market in 2003. How long do you want to wait for the industry to get a new therapy to market after the crisis has hit? Luckily, for MRSA we had at least one other efficacious antibiotic we could use. But in the case of these highly resistant Gram-negative infections, our choices are limited and not very efficacious. So how long do you want to wait?
The answer is to fix the market now – with government
funding. How much would this cost? The
US share (assuming we share the burden with Europe) would probably be something
like $1-2 billion per year over the next 10 years. Our share would decrease if
China, Japan and other Asian nations would join us. This is a paltry amount of
money compared to our national budget.
So what are you waiting for?
Are you waiting for you or one of your loved ones to encounter one of
these deadly infections personally? Are
you waiting for a more politically palatable moment to act? Like you, I am not
getting any younger. And I have children
and grandchildren I care about. I have worked in hospitals where I have had
patients with bacterial infections for which I had little or nothing to offer. Physicians
and their patients should never be put in that position. And now, you, not
anyone else – but you – are tasked with fixing this. Delay just increases the
risk of a situation that none of us wants to imagine.
I am ready, willing, and with a little help, able, to work
with you and your staffs to construct legislation that would fix the antibiotic
market. It can’t happen without you. Please help!
Sincerely,
David Shlaes
Stonington, CT
No comments:
Post a Comment